
Atlanto-occipital (AO) luxation, colloquially referred to as internal decapitation, is commonly caused by a traumatic event. With this type of injury, the ligamentous and boney structures that secure the skull to the cervical spine are damaged, resulting in instability, severe injury to the brainstem, and compression of the cervical spinal cord.1,2 More frequently described in human literature, AO luxation is the most common cervical spinal injury sustained in motor vehicle accidents.2 In comparison to the literature in humans, AO luxation has rarely been reported in the veterinary literature. Regardless of species, this type of luxation carries a high rate of morbidity and mortality due to direct neuronal damage, ischemic injury, or both.1,2 In the rare case of survival following traumatic AO luxation, prompt diagnosis and treatment, as well as appropriate supportive care, are paramount for successful patient outcome.2,3
Case Presentation
A 1-year-old female Pygmy goat was presented to Purdue University with a 1-day history of acute tetraplegia. Clinically, the goat was laterally recumbent with increased extensor tone in all 4 limbs. There was no evidence of motor function or proprioception in any limb, but all myotatic and flexor withdrawal reflexes were intact. The remainder of the neurologic and physical evaluations were unremarkable. On the basis of these findings, the patient was determined to have a neuroanatomic lesion localized to the upper cervical (C1 to C5) spinal cord segments. Considering this patient’s history, signalment, and neurologic deficits, differential diagnoses included infectious or inflammatory disease, trauma, or neoplastic process.
Diagnostics
Imaging of the patients’ cervical spine revealed dorsal luxation of the atlas from the occipital condyles with severe spinal cord compression. The owners were presented with 2 options: (1) pursue radical surgical correction or (2) humane euthanasia. Surgical risks included patient death, permanent tetraplegia, and the loss of voluntary ventilation. After weighing the options, the owners elected to pursue surgical treatment.
Surgical Correction
Surgical reduction and stabilization of AO luxation has rarely been reported in veterinary literature.1,4 There is no consensus on surgical technique or approach, although closed reduction or ventral surgical reduction is most often reported.1,4,5 Careful consideration of approach and technique was necessary, and it was decided to attempt reduction via a dorsal approach. This was due to the greater availability of cortical bone and fewer critical structures, such as the trachea and jugular vessels. One unique complication of a dorsal approach was the presence of horns, which were removed before surgical site preparation.
The goat was clipped and aseptically prepped with margins that extended from the base of the horns to the cranial edge of the scapulae and to lateral midline on either side of the neck. A midline incision was made from the external occipital protuberance to midcervical spine. The dorsal cervical musculature was elevated and the dorsal aspect of the occiput, atlas, and axis were exposed. Careful incision and debridement of fibrous tissue around the AO junction were necessary to successfully reduce the luxation. A cortical screw was placed through the atlas into the occipital condyles bilaterally to maintain reduction. Additionally, screws were placed in the dorsal occipital bone, in the dorsal aspect of the atlas, and through the dorsal spinous process of the axis parallel to the lamina. The construct was encased in polymethylmethacrylate to provide internal coaptation and maintain reduction of the joint. The incision was closed, and the patient was taken for postoperative radiography to confirm screw positioning and AO joint reduction.
The primary concern for anesthetic recovery was for the patient to voluntarily ventilate and maintain appropriate oxygenation. The goat was monitored through extubation with capnography and pulse oximetry to ensure adequate ventilation. The patient recovered well from anesthesia and did not have any evidence of neurologic deterioration after surgery.
Postoperative Nursing Care
The patient’s respiratory function was the primary concern after surgery and was assessed by observation of respiratory rate and effort, auscultation, and pulse oximetry. The patient’s recumbency was rotated to prevent complications related to atelectasis and development of decubital ulceration. Disuse muscle atrophy is a common complication in the recumbent animal, making physical rehabilitation a crucial aspect of supportive care for such patients.
Physical Rehabilitation
No current literature describes physical rehabilitation in the caprine, so the plan and goals of postoperative physical rehabilitation applied to this patient were extrapolated from canine literature and technique. A combination of superficial thermal modalities, manual therapies, and therapeutic exercises were applied throughout the rehabilitation process.
- Cryotherapy is recommended for any postoperative or acute inflammation.5 Cold results in vasoconstriction, a slowed metabolic rate, and a reduced release of histamines.6
- Heat therapy is used when soft tissue healing begins or in situations of chronic pain.7 Heat increases the rate of metabolism and allows for vasodilation, as well as relaxing muscles and relieving pain.6,7
- Massage is applied to muscles to maintain muscle condition and relieve pain. Massage promotes muscle relaxation and improved mobility and circulation.8
- Passive range of motion is used to maintain joint mobility. Range of motion reduces risk for muscle contracture, decreases edema, and promotes synovial flow.6
- Therapeutic exercises are recommended to improve limb awareness, improve core and appendicular muscle strength, and maintain posture.8 A variety of exercises are used to accomplish this.
- Underwater treadmill is appropriate for nonambulatory patients because it provides buoyancy. This minimizes weight bearing on the joints and helps to decrease pain associated with limb soreness.2 Resistance provided by the water helps to improve muscle strength.9
Within 24 hours of surgery, the goat’s neurologic function improved, with motor function present in all limbs. To get the goat back on her feet, the rehabilitation goals were to improve limb awareness (proprioception), improve balance, and improve core strength.
Cryotherapy (gel pack) was used on the incision immediately after surgery. In this case, using cryotherapy in combination with keeping the goat’s head elevated decreased muscle edema, pain, and inflammation and protected against further tissue damage. Two days after surgery, heat (gel pack) was applied to the incision and circumferentially to the neck to allow for muscle relaxation and pain reduction. Massage was performed on each limb to promote blood flow and relaxation, followed by passive range-of-motion exercises to maintain joint mobility while the goat was unable to stand.
As the patient continued to improve, weight shifting and assisted standing exercises were implemented to help the patient improve proprioception and balance and to rebuild the “mind-body” connection. During this stage of recovery, the patient was able to move all 4 limbs and could bear weight on the thoracic limbs. An exercise ball helped her stand safely and supported her whole body. It also provided a means of weight shifting to increase strength and proprioception in the hind limbs (FIGURE 1).

FIGURE 1. Exercise ball used to help the patient stand safely and increase strength in hind limbs.
In addition to use of an exercise ball, assisted standing and walking were performed by using a body sling and a patient lift (FIGURE 2). Implementing these types of rehabilitation processes improve circulation and respiration, encouraging neuromuscular function.9 While the patient is in the lift, exercises to improve core strength were also performed; these are important because they support the midsection.8 The core also plays a role in successful standing and posture maintenance.8

FIGURE 2. Body sling and patient lift.
Nine days after surgery, the patient was able to sit up from lateral recumbency voluntarily. If placed in a standing position, she was ambulatory tetraparetic with a severe proprioceptive ataxia in all 4 limbs. At this stage, underwater treadmill therapy was implemented. Buoyancy and resistance provided by the water improved her strength and proprioception (FIGURE 3).

FIGURE 3. Underwater Treadmill Therapy
The patient was discharged 14 days after being hospitalized and undergoing surgery with extensive physical rehabilitation. At discharge, she was ambulatory and able to stand voluntarily, but she was still weak and ataxic. Therefore, a harness was used to provide support. A rehabilitation plan was sent home with the patient so she could continue to work on proprioception, muscle strengthening, and balance deficits with her owners. Eight weeks after surgery, the goat was re-examined and was neurologically normal with no obvious weakness. Radiographs of her cervical spine confirmed stability of the implants and that reduction of the luxation was maintained (FIGURE 4). Additional rehabilitation was unnecessary at this time because the goat was too agile to catch easily.
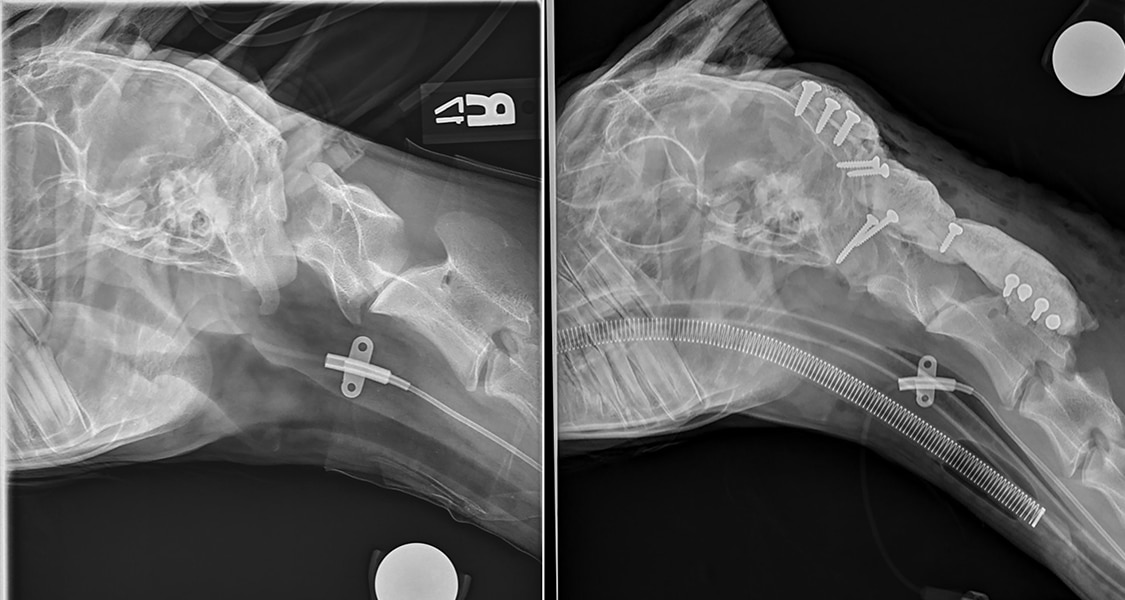
FIGURE 4. Preoperative (left) and postoperative (right) radiographs.
Conclusion
An AO luxation is a traumatic injury that is rare in the hospital setting because of the high mortality related to injury.1 This case report describes a caprine patient with this rare injury that successfully survived the initial injury and unique surgical fixation and had a successful postoperative recovery, to which extensive physical rehabilitation partly contributed. The goat continues to thrive on the farm with no obvious neurologic deficits or weakness.
References
- Buks Y, Snelling SR, Yates GD. Ventral fixation of chronic atlanto-occipital luxation in a dog. J Small Anim Pract 2011;52(9):497-500.
- Hall GC. Atlanto-occipital dislocation. World J Orthoped 2015;6(2):236.
- Dolera M, Malfassi L, Bianchi C, et al. Zygomatic arch-atlas wing stabilization in 5 dogs with atlanto-occipital dislocation. J Vet Med Sci 2016;78(6):963-970.
- Rylander H, Robles JC. Diagnosis and treatment of a chronic atlanto-occipital subluxation in a dog. JAAHA 2007;43(3):173-178.
- Sorjonen DC, Powe TA, West M, Edmonds S. Ventral surgical fixation and fusion for atlanto-occipital subluxation in a goat. Vet Surg 1983;12(3):127-129.
- Levin D, Marcellin-Little DJ, Millis. Rehabilitation and physical therapy. Vet Clin North Am Small Anim Pract 2015;45(10):29-41.
- Millard RP, et al. Effect of warm compress application on tissue temperature in healthy dogs. Am J Vet Res 2013;74(3):448-451.
- Millis D, Levine D. Canine Rehabilitation and Physical Therapy, 2nd ed. Philadelphia: W.B. Saunders; 2014.
- Chiquoine J, McCauley L, Van Dyke JB. Aquatic therapy. In: Canine Sports Medicine and Rehabilitation. Zink MC, Van Dyke JB, eds. Ames, IA: Wiley-Blackwell; 2013:159-164.